Blog by Sumana Harihareswara, Changeset founder
My Current Approach To Reducing My COVID Risk
I follow a few main principles to reduce my risk of catching COVID-19:
- Avoiding sharing unfiltered air with people outside my household
- Noticing how safe I am and raising precautions accordingly
- Focusing on protecting myself over protecting unmasked people (in general)
- Spending money
In this post, I detail those principles as well as my specific protocols (masking, ventilation, self-testing, and so on), including links to examples and product vendors.
Last month, the US ended the public health emergency and national emergency declarations regarding COVID-19. Many of the subsidies, protections, and other supports that helped us prevent COVID-19 transmission have gone away. Masks are optional on Amtrak, on airplanes in the US, and on my (New York City's) transit system. And -- anecdotally -- many people have stopped masking in other shared indoor spaces or otherwise trying to reduce their exposure.
Some of us are still trying to avoid catching COVID-19, and we are, more than ever, on our own.
I'm writing this post to describe my overall approach to reducing infection risk. Please feel free to link! I hope it helps other folks with similar goals. And I can point to this instead of sending it as an email to people I'm about to visit.
I follow a few main principles:
- Avoiding sharing unfiltered air with people outside my household
- Noticing how safe I am and raising precautions accordingly
- Focusing on protecting myself over protecting unmasked people (in general)
- Spending money
Below, I'll explain those, and I'll share my specific protocols in detail (masking, ventilation, self-testing, and so on), including links to examples and product vendors.
Principles
My overall approach:
Shared air
I avoid sharing indoors air, especially unfiltered air, with people outside my household. I mask in those shared spaces; "one-way masking" (I'm masking but they aren't) is less effective than all-way masking, but it's still something. When possible I substitute alternative ways of interacting with others, such as meeting outdoors, or (if one of us has had a recent exposure) phone or videocalls. Sometimes I avoid a subway or bus ride by bicycling instead.
If I'm meeting others indoors, I try to increase filtration and ventilation with air filters, open windows, and fans, and I wear high-filtration masks.
Checking my safety and raising precautions
I use safety assessment tools to determine appropriate precautions; sometimes I am willing to do more work and take on more inconvenience when the danger is greater. Factors I consider include wastewater surveillance testing data in the US overall and in my region, test positivity rates, and carbon dioxide levels in indoor spaces (as a proxy for unventilated exhalations). I sometimes play with microcovid.org's calculator to better understand what I can do to make a situation relatively safer.
Protecting myself over unmasked people
I sometimes am willing to wear a valved mask (that is, a mask where the air I inhale is filtered, but the air I exhale is not). Sometimes a valved mask can provide me with higher protection with less discomfort than can a nonvalved mask. Criteria: I am in a large public group, nearly no one around me is wearing a mask, masks are not mandated, and I am not in a healthcare setting. (I am not 100% committed to this reasoning. In particular, one person I know who takes pretty similar precautions to mine is very interested in preventing transmission to others, on the theory that he particularly wants to do his bit to prevent the mutation of the virus into harder-to-fight variants. That seems pretty sensible!)
A similar principle also applies to how much time I spend protecting myself and my circle of loved ones directly versus how much time I spend on advocacy or similar work to try to protect the general public. I do, for instance, contact event organizers in my industries and hobbies to ask about ventilation and air filtering. But I have not been spending time on, e.g., calling my federal representatives to lobby for unlikely policy changes.
Spending money
Some additional protections cost money, and I have decided that it's worth maybe a few thousand dollars per year to not catch COVID, or delay catching it for a few more years as we discover and refine treatments. I do not want to catch COVID nor pass it on to others. Even mild cases lead to increased risk of heart attack, stroke, type II diabetes, autoimmune diseases, and probably other conditions. The virus can stick around in the body for years. I especially do not want to develop Long COVID; I have a few friends with Long COVID and it has been extraordinarily damaging to their lives (including in some cases their careers), and we are just now learning some ways to reduce the risk of Long COVID among people who get infected. So the investment is worth it. I am lucky to be able to make this investment.
Protocols
Here's a summary of what I do to mitigate COVID transmission risk. I also specify what I would ask of you if we're seeing each other (at the end of the Vaccination, Masking, and Self-Testing sections).
I've now used these to help keep me safe while seeing local friends, travelling via air, train, bus, and car, taking care of family, participating in PyCon US and WisCon this year (including speaking onstage), and so on; I have not yet caught COVID (and I did take an antibody test to check).
- Vaccination: Get every booster as soon as possible.
- Air quality and ventilation: Go outdoors or use fans, filters, and breaks, and use a carbon dioxide monitor to check.
- Masking: N95, N99, or P100. More protection when I'm at more risk.
- Self-testing (antigen and NAAT/molecular) and PCR: Self-test if I have symptoms, am seeing someone indoors in a private space, or am at a big event.
- Nasal spray: Enovid before and after indoors time with strangers.
- Staying apprised: Wastewater and test positivity data, plus general COVID news.
- In case I catch it: Isolation, Paxlovid, metformin, Enovid, and rest.
- Returning from a trip: Isolation, ventilation, and testing.
Vaccination
I get every COVID-19 mRNA vaccine booster as soon as it's available to me.
What I ask of friends and colleagues before we meet in person: I realize upon writing this that I have not been asking people whether they're vaccinated and whether they've gotten their latest booster shot before I meet them, because I assume that they have, and because it feels insulting to check. I'll have to consider this.
Air quality and ventilation
Fresh air with a breeze helps wash viral particles away, so I try to meet others outdoors as much as possible.
When I'm indoors with others: freshly cleaned and circulated air is safer, so I try to keep windows open, and turn fans on. If I have a choice of transport methods, I may choose, for instance, an aboveground MTA train instead of a belowground one. On car rides I try to get fresh air circulating when possible.
To measure air quality, I use an Aranet 4 carbon dioxide monitor. The Aranet 4 costs USD$249; here's a 20% off coupon. As Aranet's marketing material summarizes:

Aranet 4 carbon dioxide monitor measuring air CO2 on an underground New York City MTA subway train in June 2023, showing 955 ppm.
CO2 level as a proxy for ventilation quality: Monitoring CO2 in public spaces helps to encourage proper ventilation. CO2 is a gas produced when we exhale. So, the higher CO2 in the room, the more you’re breathing air that someone else has already exhaled. Therefore, monitoring CO2 levels provides warnings about the air quality deteriorating.
[Ugh subscripts for the "2" aren't working, argh.]
Fresh outdoors air is in the 420-470 CO2 parts per million range. General rules of thumb: up to about 800-1000 ppm is somewhat safe ("green"); 1000-1600 ppm is iffy ("yellow"); above 1600 is bad ("red").
The Aranet 4 measures carbon dioxide in the air. It has an e-ink screen to display the current reading and what range it's in, and you can configure it to audibly buzz if it goes over a particular threshold. The sensor also measures humidity, temperature, and barometric pressure. You can set it to sample the air every 1, 2, 5, or 10 minutes, to balance between fresh frequent measurement and saving the battery. The device runs for like 6 months on 2 AA batteries.
And it comes already calibrated from the factory so you don't have to do that yourself. I recently hung out with a friend who also has an Aranet 4, and we each got out our device. Our measurements were within 1 ppm of each other.

2 Aranet CO2 monitors reading 465 and 466 ppm, on a breakfast table outdoors in June 2023 in New York City.
There's a phone app (connecting over Bluetooth) to check trends over time, change how frequently it samples the air, and so on. You can download a CSV so you can do data analysis yourself. There are device firmware updates every several months. Neither the firmware nor the app is open source and I am grumpy about that.
The Aranet 4 device weighs a few ounces. I keep ours in a little canvas pouch that I attach with a carabiner to my belt loops or my handbag. (Note: It's not impact-resistant, and if it knocks against something hard, the case might slip and let the batteries out, which means you lose all the readings you hadn't yet synced to your phone.)

Aranet CO2 monitor reading 736 ppm while I am in the audience for a PyCon US keynote in April 2023.
Big conference centers and well-maintained transit (such as BART) keep even very populated rooms under 800 ppm.
Indoors conversations can get into the 1200 range in badly-ventilated rooms, such as hotel rooms without openable windows.
Airplane rides are usually someplace 1000-1800 while in midflight, but more like 1400-3500 while taxiing, sitting on the tarmac, or during takeoff and landing.
The worst ventilation, I've found, is on car rides where we haven't adjusted fan settings to bring fresh air in. I've been on one-hour car rides where the CO2 level went near 6,000 ppm.
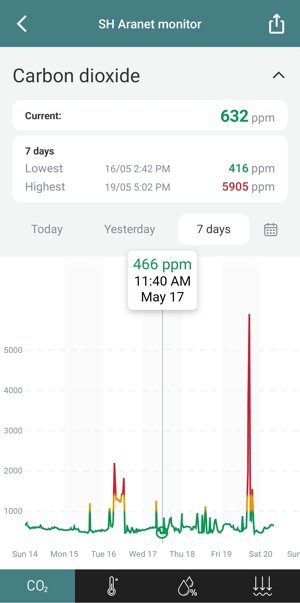
Aranet CO2 monitoring app screenshot from one week in May 2023. Almost all readings are in the green range, under 1,000 ppm. A few hours in the yellow and red ranges, about 1,000 to 2,100 ppm, are during airplane travel. The 5,905 ppm peak is during a car ride.
Do note: if you're running an air purifier in a space but it's not bringing fresh air in, then it'll filter viral particles but won't replace carbon dioxide with oxygen. And thus the climbing CO2 numbers will be somewhat misleading as a proxy for COVID safety.
I prefer to spend shared time with others outdoors, and while we're indoors, I modify how physically close we are partly based on others' recent exposures. I can play with microcovid.org's calculator to better understand what I can do to make a situation relatively safer, by fiddling with physical spacing, duration, speaking volume, etc. As this guide to protecting yourself from aerosol transmission summarizes, I want to avoid:
- Crowded spaces
- Close proximity to others
- Low ventilation environments
- Long durations
- Places where people are not wearing masks
- Talking, and especially loud talking / shouting / singing
- High breathing rates (e.g., indoor aerobic exercise)

Aranet CO2 monitor reading 1626 ppm at an indoors concert, December 2022. On its left: the canvas pouch I carry the device in.
And that "long durations" item matters! As an April 2023 paper ("Airborne disease transmission during indoor gatherings over multiple time scales: Modeling framework and policy implications") explains, break times during and between meetings reduce the room's viral load a lot.
i) high air filtering efficiency becomes more important as meetings extend, as the cumulative virus stock critically increases when the group size is large
ii) splitting the meeting to allow air filtering during a long enough break is better than splitting the crowd for two full-session meetings
iii) We go beyond the well-known role of face masks in limiting disease transmission and quantify how their benefit trades off against other measures such as better air filtration and intermeeting breaks
iv) intermeeting break times dramatically reduce the room’s viral load, potentially equalizing masks and testing effects. Allowing break times between meetings modulates the room’s viral load.....
.... ventilation and break times are critical in preventing high viral load levels. Moreover, we found that their impact would equal or exceed that of masking and moderate isolation of infected individuals.
Also: If you own your own home or business, consider installing an ultraviolet light in your air system to sanitize the air.
Masking
Outdoors, I usually don't wear a mask. If I'm in a group or crowd for more than a few minutes, I'll limit my unmasked time (e.g., eating quickly and then putting a mask back on). Or, if I'm talking at length with one person and either of us prefers that I mask (e.g., I've just come back from a trip, or they're immunocompromised), I'll mask. Outdoors I wear a KN95 or an N95.
I mask indoors in shared spaces, including during car rides, with anyone outside my household. (My household is me plus my spouse.) In a world where nearly no one else masks, I need to rely on one-way masking, which means I wear an N95 or something with a higher filtration rating, as surgical masks and KN95s are usually not protective enough for my liking.
My default mask/respirator is an N95. I generally use a 3M Aura (USD$42.57 for a pack of 20 from Home Depot) or a duckbill-style Kimberly-Clark mask (USD$22.69 for a box of 20 from Betty Mills) because those fit well enough that my eyeglasses don't fog up. I keep procrastinating on doing a proper fit test and figuring out which masks fit me best, and it's pretty important to do so! Maybe writing this will get me over that hurdle.
Me wearing a 3M-brand Aura N95 mask.
If I'm sleeping in a place where I can't close the door between me and untested others, I do mask while sleeping. I find the Kimberly-Clark duckbill-style N95s comfortable enough to sleep in.
I also mean to investigate the 3M VFlex, which has pleats shaped to make breathing easier, and the Readimask, which seals to the face without straps and is thus useful for dentist appointments. I bet that's also worth trying for sleeping.
Me wearing a duckbill-style Kimberly-Clark N95 mask.
If I'm doing public speaking indoors, I may use a clear JelliM mask (under $USD30) which is akin to a surgical mask [Edited 21 June 2023: I'd previously said it's at a similar protective level to a KN95, but I'd misremembered a friend's assessment], and then switch back to a more protective mask once I'm off the stage. The idea is to help people who need to read lips to better understand what I'm saying. I'm not sure how effective the JelliM has been at this goal. I think there is a little tendency to fog up, and bright stage lighting can cause glare and block the view of my lips, and the sound of my voice can get a bit echoey or muffled (as in the audio for the "Argument Clinic" recording).
Me wearing a JelliM mask. There's an opaque white border around the chin, cheeks, and nose, but the viewer can see my mouth clearly.
My default mask is an N95, but for airports, airplanes, and crowded public places I bring my Aranet 4 CO2 monitor, check it, and graduate to more protective respirators if the CO2 levels go dangerously high. If CO2 is in the yellow range I often go up to a disposable valved N99 (USD$26.15 for 20 masks at Betty Mills).
An N99 has individually adjustable elastic straps, and soft material around the mouth and nose area, ensuring a closer fit than I usually get with an N95. It is also valved, meaning that it filters incoming air but not outgoing exhalations. (I believe I've seen some headlines saying that the level of filtering for outgoing breath is not zero, maybe at about the level of a surgical mask. [Edited 21 June 2023 to add:] Reader foxfirefey pointed me to this NIOSH study: "Filtering Facepiece Respirators with an Exhalation Valve": "FFRs with an exhalation valve provide respiratory protection to the wearer and can also reduce particle emissions to levels similar to or better than those provided by surgical masks, procedure masks, or cloth face coverings.") So, when I wear an N99, I'm choosing to protect myself over others; see my principles for when I might do this.
As with N95s, I reuse an N99 till the straps start giving out. I find N99s pretty comfortable.
Me (left), wearing an N99 valved mask, standing next to NYC Councilmember Shekar Krishnan in June 2023.
If the CO2 is in the red range, I wear a P100-level respirator. I use a 3M half-face which cost USD$35. Like all P100s (I think), it is elastomeric, which means that it has soft bits around the mouth-and-nose area to form a good seal with the skin, and has replaceable filters.
This P100 has an exhalation valve, which I have covered up with a piece of KN95 or surgical mask material and some tape so that I am protecting others by filtering my exhalations. I keep meaning to buy the official 3M exhalation valve filter and install it (about USD$10 each but seems to only come in a pack of 6).
I've had this P100 for going on 2 years now, and have replaced the filters a few times (maybe USD$10-20 per pair). I find it comfortable enough that I have slept many hours while wearing it on trains and airplanes. I do make sure to do a quick positive and negative fit test each time I put it on (inhaling and exhaling while covering the filters and exhalation valve) to ensure good fit. Sometimes I do adjust the straps too tight and get a bit of a headache after 40 minutes, and then need to carefully loosen them an iota.
I am thinking about getting a smaller P100. I'd like for the filters to not block as much of my vision, and for the entire kit to pack up smaller in my handbag. And it may be occasionally helpful to wear something that isn't quite as attention-catching, although I don't mind being eye-catching. A friend likes the Comfort-Air Nx (USD$31.25), which does filter outgoing breath. Another friend likes this low-profile Klein P100 (about USD$30) , but warns that the replacement filters can be harder to find.

Me wearing a 3M half-mask P100 respirator, December 2022, at a concert. This is the concert where the CO2 reading was 1626 ppm.
If I need to visit someone who has an active COVID infection, then I also wear eye protection (these goggles cost maybe USD$20).

Me wearing a 3M P100 half-face respirator and goggles.
Socializing with food and drink: Outside my home, I eat & drink outdoors, or in a room by myself with the door closed and the window open. In a pinch I can lift my mask indoors to take bites and sips; I'm more ok with this if the CO2 reading is lower than about 600 ppm. I am fine eating and drinking outdoors with friends who have my own or a somewhat looser standard of caution.
What I ask of friends and colleagues: Mask in indoors public/shared spaces with me, except while eating/drinking. (Exception: If I am visiting someone in their home, I generally do not request that they wear a mask in their own home.)
If we want to be able to unmask indoors together, such as for meals, then I check that we've both had negative rapid tests within the last ~12 hours, and I limit the time I am unmasked (for instance, putting a mask back on between courses of a meal). I'm more willing to unmask if ventilation is pretty good (say, under 700 ppm CO2). I'm also less likely to be willing to unmask if either of us has been in high-exposure situations in the past five days, but that can be pretty contextual.
If I'm visiting friends for more than a day and we'll be spending many hours sharing air, I often request that they avoid unmasked indoors time outside their household, starting about three days before I arrive.
Self-testing (antigen and NAAT/molecular) and PCR
If I'm feeling symptoms, I'll take a rapid home test, usually an antigen test but sometimes a higher-accuracy NAAT (a.k.a. "molecular test").
If I'm not feeling symptoms then my testing is generally before or after seeing other folks indoors.
Prior to seeing someone else indoors in a private space: I self-test at home.
If I am travelling to a public group event such as a convention, I bring several tests. I self-test before leaving my home and every day, or every alternate day, of the event. Then, about five days after returning from travel, I get a free PCR test, which is the gold standard for accuracy, via New York City's COVID Express sites.
Since antigen tests are cheaper than NAATs, I use antigen tests most of the time. I use NAATs when the stakes are higher or when I consider my likelihood of infection or transmission to be higher, e.g., if I'm about to see someone who's immunocompromised, or have had a lot of indoors exposure to strangers recently, or want to unmask indoors with someone in a low-ventilation room.
Free and subsidized testing: In the US there are still ways to get tested for free. Here's the CDC's test locator. And: if you bought at-home tests before May 11th, 2023, you can likely submit receipts for reimbursement to your health insurer.
Your old tests may still be good: If you have rapid tests that say they've expired, check this FDA updates page to see if their expiration dates have been extended!
Buying antigen tests on sale: You can order big multi-packs of antigen tests from Betty Mills for pretty cheap. And a friend passed on a deal from their friend K:
"The cheap rapid tests are at maskwholesale.eu. The more tests you buy, the cheaper shipping comes out to be, so if you order over 120 tests, they end up being around $1 each. My friend J recommends Green Spring brand tests based on the data they have found."
J is immunocompromised, so K trusts their research into this stuff, but you can of course verify. The shipping may be a bit high for individuals, but it worked out well for the bulk order for our house.
As siderea further wrote up: "They ship world-wide via DHL. They're selling, e.g. Flowflex for EUR 0.83 each (less for bulk orders!) while shipping to the US or Canada is about EUR 50 for up to 10kg (EUR 20 within the EU, EUR 35 to the UK, EUR 65 to AU). They have many, many brands and types of tests, including combined Covid + Influenza A/B tests(!)."
[Edited 21 June 2023 to add]: Check again at the end of the results window: Home antigen tests often instruct you that the soonest you can check results is 15 minutes, and that the longest you should wait to check the results is 30 minutes. I check at the 15-minute mark and then again at the 30-minute mark, because very early positive results sometimes take more than the minimum results time to show up. I read Jessi Grieser's experience last year: "my home test ... took almost a half an hour to turn up the very faint positive line. 15 minutes was not enough to test positive--had I been using the test to determine 'can I walk in the house to see grandma' I would've been wrong."
[Edited 21 June 2023 to add]: Consider swabbing throat + nose: In some countries the rapid antigen test procedure includes doing a throat swab. I get the sense that adding a quick swipe of the back of the throat before swabbing the nostrils is likely to help catch the more recent variants (since early 2022). If I need to do an antigen test and I haven't eaten or drunk anything in the last hour or so, I also swab my throat. It seems to make the control line a little fainter but otherwise doesn't get in the way.
Higher-accuracy home tests on sale: NAATs (Nucleic Acid Amplification Tests) are more accurate than antigen tests; false negatives are less [edit 2023-06-16: I had accidentally said "more"] likely, and they're better at catching early cases. PCR (polymerase chain reaction) is one example of a NAAT.
Another NAAT is the Lucira CHECK-IT disposable at-home test. It uses loop-mediated isothermal amplification (LAMP) which is a particular type of NAAT. Lucira's test takes 30 minutes to run and display the results - no app needed. The no-transmission 2023 Honeycomb offsite included frequent rapid COVID testing using Lucira kits. (It's wasteful to throw away an entire piece of electronics for every test; I'd love to know of hackerspaces that want used tests to hack on.)
Lucira's tests used to cost about USD$80 each. Then they were running low on cash and started selling them for more like USD$40 each. Then Lucira filed for bankruptcy and then was bought by Pfizer, and paused production, and now you can't buy those tests from their site or from Amazon anymore.
But! vaulthealth.com has those Lucira rapid COVID tests for sale for USD$12.50 each. (As of right now, mid-June 2023.) They have expedited delivery available, and, there's a 25% coupon on top of that with discount code SPRING23 . The catch is that these are tests with expiration dates in July (originally marked as expiring in January 2023, then extended to late July). But if you have exposure risks over the next 6 weeks, this is actually an excellent deal.
I ordered and successfully received several. I had not ordered from Vault Health before, but found out about them by calling Lucira and finding out that Vault is one of their distributors. (The Lucira customer service rep told me that they do plan to resume production but he couldn't give me an exact date.)

A negative Lucira rapid COVID test. A sealed test tube containing purple liquid sits in a slot at the top of the white device. The base of the device includes indicators: "Ready", "Done" (green light), and COVID-19 "Positive" and "Negative" ("negative" has the green light).
I've used Lucira tests without difficulty in the past. Then, with the ones I ordered from Vault, things mostly worked fine, but I've had a few problems:
- I once got an invalid result (all of the lights flashing) instead of a valid result. I figure that is likely because of a fumble made when placing the vial (I did see a drop of fluid spill into the aperture), or possibly because I attempted to use the same pair of AA batteries for the 3rd test in a row, instead of using a fresh pair each time (each kit comes with a fresh pair of AA batteries to use, but a battery tester demonstrates that running the test once still leaves plenty of charge on the batteries).
- I once got a positive result, which was later that day demonstrated to be erroneous by two separate PCR tests (including a deep nasal passages swab). This of course royally screwed up the course of my morning, and now I am a little suspicious about whether that particular batch of tests might be especially susceptible to false positives. Maybe Vault didn't store them correctly, or maybe I left them someplace too hot as I schlepped them around the Bay Area in my luggage, or maybe the extended expiration date comes with sensitivity degradation.
- Maybe 1/4 of the kits had a minor issue: when I was peeling the seal off the test tube, the tiny plastic handle wasn't adhering very well to the foil seal, so I had to carefully find a way to peel the foil off with my fingernails or something. Possibly some adhesive degraded over the months.
Lucira's other distributor is Peach Medical, which does have some of their NAAT/molecular COVID tests in stock at USD$34-$45 each ($34 for ones that expire in August, $45 for ones that expire in October). Peach also has Lucira's COVID + Flu test kits in stock, but only in a USD$1,440 pack of 24 tests.
Cue: We don't know whether or when Pfizer will resume producing and selling Lucira tests, and they might bring the price back to like $80 each, plus I dislike the physical waste anyway. So I'm thinking of buying a Cue Health device & cartridge subscription. Cue is also a NAAT. One Cue unit costs USD$99 and the individual disposable test cartridges cost USD$50 each, and it does require the user install a phone app to run tests and read results. Bleh. But I know a lot of people who have and like the Cue.
What I ask of friends and colleagues: if we're going to meet indoors for more than about an hour, or if we're meeting indoors and you've had a lot of exposure over the last 5 days, self-test with a rapid antigen or molecular test within the day we meet, before we meet. If you develop any symptoms within like 5 days of our meeting, I'd like for you to self-test as well, if that is easy/feasible for you, and to inform me if you test positive.
Nasal spray
Researchers are looking into sprays that can make it harder for viral particles to survive in the nasal passages. I've read a bit about Enovid and similar nasal sprays. How Enovid ("SaNOtize Nitric Oxide Nasal Spray (NONS)") works: when you activate the spraying mechanism, the ingredients in Enovid turn into a combination citric acid-nitric oxide spray which kills virions. It's approved by the medical authorities in Israel to sell in pharmacies there, so a friend visited Israel and brought some Enovid back for me.
US residents and some others can also purchase Enovid online for about USD$50 per 25 mL bottle, which is about 200 doses. I used up a bottle over about 8-10 weeks that included a bunch of travel.
As I understand it, the published research supports the conclusion that, if you catch COVID, Enovid usage will reduce the duration and intensity of the acute phase of the infection. Beyond that, a bunch of us are like "it stands to reason that spraying it in your nose before and after an exposure, it'll reduce the chances of getting infected at all??!!" and so we are prophylactically snorting it before and/or after plane rides, indoors time with strangers, etc. It stings a bit on the way in but otherwise I have felt no perceptible side effects.
[Edited 21 June 2023 to add]: Reader ungemmed shared with me the fact that nitric oxide/dinitrogen oxide (NO/N2O) can affect uptake of vitamin B12. When ungemmed was using it prophylactically 4-5 days per week, "it seemed to exacerbate some B12 deficiency symptoms I was independently having...Suspect it's fine for most people, but something to watch if one is using it regularly."
This is probably the most eyebrow-raising item in this post; I am aware that snorting a medication that is not approved by the US Food And Drug Administration puts me in rather mixed company. I assert to you that I have not turned into an ivermectin aficionado or something like that. But then again, I would say that, wouldn't I.
Staying apprised
I try to stay apprised of the current level of COVID prevalence in my area and of new threats, prevention tactics, and treatments.
Wastewater testing data (COVID rates in sewers -- excellent because it isn't biased by whether someone actively seeks testing): I sometimes visit Biodata's dashboard covering the US, its regions, and several cities, and Boston's MWRA as a reasonable proxy for New York City since NYC's official wastewater testing data is updated far less frequently. Also I recently learned of WastewaterSCAN which also looks very useful, especially as it includes NYC.
Test positivity rate and similar data for New York City specifically: the tracking charts run by THE CITY.
General news about COVID: I pay consistent attention to THE CITY, the New York Times, and various bloggers and commentators I follow via Dreamwidth, Mastodon, and syndication feeds, such as siderea and Erin Kissane. If I am trying to understand fresh news about COVID risk or research, I check for commentary by Kissane and siderea, then go to STAT News, Your Local Epidemiologist (Katelyn Jetelina), Bob Wachter, and Eric Topol.
In case I catch it
If I catch COVID, I want to reduce the chances of transmission to others, and I want to reduce the chances of developing Long COVID. Therefore:
- Isolation: I'd get into a room as isolated from others' air as possible, and ventilate and filter the air to keep viral load low. This might mean a hotel room.
- Paxlovid: Before travelling in the US, I look up local Test-To-Treat pharmacies, hospitals, urgent care facilities, and telehealth. For instance, if I had tested positive while in Madison for WisCon, I would have used Wisconsin's telehealth system to get a Paxlovid prescription ASAP.
- Metformin: We now know that metformin, when taken during the acute phase of COVID infection, significantly reduces the chances of developing Long COVID. (Eric Topol writes: "unless or until there are data to the contrary, if I got Covid, I’d take metformin for 2 weeks at the doses used in this trial") So I would request my physician prescribe me metformin.
- Enovid: I'd snort Enovid nasal spray to reduce the duration and intensity of infection.
- Rest: To help prevent developing Long COVID, I'd try to physically and mentally rest as much as possible for the first two weeks of the infection.
I would also probably follow up on crowdsourced recommendations such as an alkaline diet and dietary supplements.
Returning from a trip
I don't want to transmit COVID to my spouse. So, when I return from high-exposure travel (such as airplane trips), we use isolation, ventilation and filtration, and testing to reduce transmission risk.
For about the first 5 days after I return, I mask in shared spaces with an N95; Leonard often masks with a KN95. We open the windows as much as possible, and/or use multiple standalone air filters/purifiers (we've bought a few, ranging from about USD$20-150 each). We sleep in separate beds, or I keep an N95 mask on and we ensure good ventilation while we sleep. Often we eat together outdoors, or I eat in a separate room with the door closed. For some meals, if I have no symptoms and the CO2 level is under 600ppm, we'll take off our masks to eat together in shared indoors air.
During those 5 days, if I develop any symptoms, I take a rapid test.
About five days after returning, I get a free PCR test via New York City's COVID Express sites. That result comes back within 24 hours -- often in just 2-5 hours -- and I consider that a "we're clear" signal. We unmask and smooch!
Also: When I return home from going outside, I wash my hands, and try to scrub for 20 seconds each time. We now know that transmission of COVID via surfaces is pretty rare, but it's a good habit for avoiding various other germs so I'm keeping it up anyway. Similarly, I'd already had a bit of a pre-pandemic practice of switching from "clothes I've worn while sitting on trains or other public furniture" to "home clothes" upon coming home from outside, and now it's somewhat more rigorous. This is more about mpox, and a general feeling of domesticity, than about COVID.
Further reading & concluding thoughts
Till I move off Pinboard, I do bookmark a bunch of resources and tips using the covid-19 tag there. For instance, WisCon's 2022 post-con report details the many steps they took to mitigate spread, including buying and building air purifiers. And just today I saw Erin Kissane point to some promising mouthwash research.
I feel fortunate that I can learn from so many researchers and educators about how to keep myself safe, and that people like me form enough of a market that vendors continue to create and sell us tools. It seems more constructive to concentrate on that gratitude and self-efficacy than to focus on how awful it is that we're missing the opportunity to collectively, as a civilization, protect ourselves en masse.
By some estimates, only 6% of the US population had not yet been infected by COVID by mid-November 2022. Others suggest it's more like 15% of US residents who have been able to avoid infection so far. I aim to continue to be one of this fraction. I hope these tips can help you avoid getting infected or reinfected. I know I've written a freaking tome here but it really usually doesn't take up more of my life than any of the other bits of regular hygiene do; once the gear and the habits are in place, it's a fairly small marginal cost. And I'm pretty sure it's worth it.
Comments
Jerome
18 Jun 2023, 13:47 p.m.
Sumana Harihareswara
https://harihareswara.net
28 Jun 2023, 19:05 p.m.
Thanks, Jerome!
Coral Sheldon-Hess has written about their risk assessment as an immunocompromised person, their approach to mitigation, and several mask recommendations. They note:
"Sumana, if you see this, you might consider adding 'hydrate beyond all reason—no really, even more than that' to your list of what to do in case you get COVID-19...."
and so I'm noting that here -- thanks, Coral!
People have discussed this post in the Fediverse (mostly on Mastodon) with some useful questions and recommendations, especially on masks. And the Dreamwidth discussion includes further notes on Enovid and on masks.

I've really kind of slipped on keeping up to date with current covid trends and info, so this post is great–truly appreciated!